
When a worker gets hurt on the job, getting the right medication is critical. But in today’s workers’ compensation system, generic substitution isn’t just a cost-saving trick-it’s the standard. More than 89% of prescriptions in workers’ comp cases now use generic drugs, and that number is climbing. Why? Because generics work just as well, cost a fraction of the price, and are backed by strict federal rules. Yet many injured workers-and even some doctors-still hesitate. Let’s cut through the noise and explain exactly how generic substitution works, why it matters, and what you need to know if you’re dealing with a work injury.
How Generic Substitution Works in Workers’ Comp
Generic substitution means replacing a brand-name drug with a chemically identical version that’s been approved by the FDA. It’s not a guess. It’s science. The FDA requires generics to have the same active ingredient, strength, dosage form, and route of administration as the brand-name drug. They must also prove they’re bioequivalent-meaning they get absorbed into the body at the same rate and to the same extent. This isn’t a loophole. It’s a legal requirement under the Hatch-Waxman Act of 1984, which created the modern framework for generic drug approval.
In workers’ compensation, this isn’t optional. Most states have laws or regulations that require pharmacies to substitute generics unless the treating doctor specifically writes “dispense as written” or documents medical necessity. For example, Tennessee’s 2023 Medical Fee Schedule says plainly: “An injured employee should receive only generic drugs… unless the authorized treating physician documents medical necessity for the brand-name product.” That’s not a suggestion. It’s policy.
Pharmacy Benefit Managers (PBMs)-like OptumRx, Express Scripts, and Prime Therapeutics-run the backend of this system. They set formularies, which are lists of approved drugs. If a drug has a generic version on the formulary, the system automatically substitutes it. You don’t get to choose unless there’s a real medical reason not to.
The Cost Difference Is Staggering
Here’s the hard truth: brand-name drugs are getting more expensive. Over five years, the list prices of the most commonly used brand-name drugs in workers’ comp jumped 65.5%. Meanwhile, the cost of generic versions dropped by 35%. Compare that to milk and bread, which rose just 7.4% in the same period. That’s not inflation-it’s exploitation.
Generic drugs typically cost about 20% of the brand-name price. A $100 brand-name painkiller? You can get the exact same active ingredient in generic form for around $20. That’s an 80% savings. Multiply that across thousands of claims, and you’re talking billions of dollars saved every year. Workers’ compensation pharmacy costs make up about 20% of total medical spending in these systems. Without generics, those costs would be unsustainable.
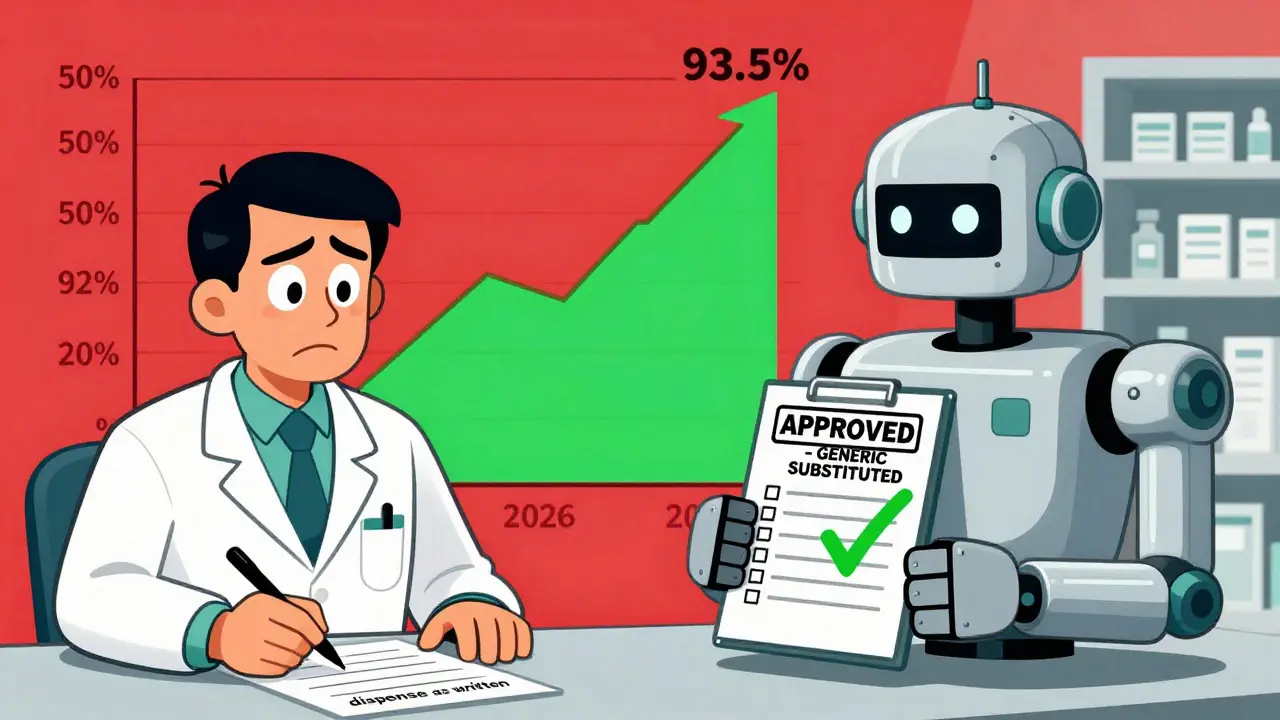
States with strong formulary rules are seeing results. California’s drug formulary achieved 92.7% generic utilization by 2022. Colorado’s 2023 rule requires 95% generic use for all drugs on its formulary-effective January 1, 2024. By 2025, experts predict generic use in workers’ comp will hit 93.5%. That’s not a trend. That’s a transformation.
Why People Still Doubt Generics
Even with all the data, skepticism lingers. A 2019 survey found that 68% of injured workers believed brand-name drugs were better. Why? Because of marketing. Ads, packaging, and brand names create the illusion of superiority. But here’s the reality: a generic ibuprofen tablet has the same active ingredient, in the same amount, as Advil. The only differences are the color, shape, or inactive fillers-none of which affect how the drug works.
Nurse practitioners in occupational health report the same thing: patients often refuse generics. “I’ve had workers say, ‘I’ve always taken the blue pill,’ or ‘My doctor said the brand is stronger,’” says one clinician in a 2022 NursingCenter.com article. The response? Show them the FDA’s bioequivalence standards. Explain that the same manufacturing rules apply. And remind them: if the generic didn’t work, it wouldn’t be approved.
Still, some concerns are valid. A tiny fraction of drugs-less than 2%-have a narrow therapeutic index, meaning the difference between a helpful dose and a harmful one is very small. For drugs like warfarin or levothyroxine, switching between brands or generics can require closer monitoring. But even then, the FDA approves generic versions only after proving they’re stable and safe. Most workers’ comp systems handle these cases with extra care, not by avoiding generics altogether.
State Laws Vary-But the Trend Is Clear
Not every state enforces generic substitution the same way. As of 2026, 44 states and the District of Columbia have laws or rules that allow or require generic substitution in workers’ comp, as long as it’s medically appropriate. Some, like Tennessee and California, have strict formularies and require doctors to justify brand-name use. Others are looser, with no formal list, and brand-name drugs are still prescribed more often.
But even in permissive states, the market is shifting. PBMs control about 65% of the workers’ comp pharmacy market. They don’t negotiate with doctors-they negotiate with manufacturers. And they’ve learned that generics are cheaper, more predictable, and easier to manage. So even if a state doesn’t mandate substitution, the system pushes toward it anyway.
Virginia, for example, has broader language that allows exceptions for occupational diseases under unusual evidentiary standards. But that’s the exception, not the rule. The overwhelming majority of states are moving toward tighter control-not away from it.
What Happens When Generics Don’t Work?
It’s rare, but it happens. A worker might feel a generic drug doesn’t help as much. Maybe they’ve had bad experiences in the past. Or maybe they’re one of the few people who react differently to inactive ingredients. In those cases, the system isn’t rigid. Doctors can still prescribe brand-name drugs-but they have to document why.
That means more than saying, “I prefer the brand.” It means: “The patient had an allergic reaction to the filler in the generic version.” Or, “The patient tried two generic versions, and both caused nausea.” Or, “The drug has a narrow therapeutic index, and the brand has a proven stability profile in this patient.”
Without that documentation, the claim gets flagged. The pharmacy won’t fill it. The insurer won’t pay. It’s not about preference-it’s about proof.

What’s Next? Biosimilars and Personalized Medicine
The next wave is coming. Biologic drugs-complex medications made from living cells-are becoming more common in workers’ comp, especially for chronic pain and inflammation. These drugs used to have no generics. But now, biosimilars are entering the scene. These aren’t exact copies, but they’re designed to work the same way. Texas led the way in 2022 by implementing the first workers’ comp biosimilar substitution protocols.
Looking ahead, pharmacogenomics could change everything. That’s the science of how your genes affect how you respond to drugs. In the future, a simple DNA test might tell a doctor whether a worker is likely to metabolize a certain painkiller slowly or quickly. That could mean customizing treatment-not just picking a generic, but picking the right generic for that person.
But for now, the rule is simple: if a generic exists, it’s the default. Unless there’s clear medical evidence it won’t work, the system moves forward with the cheaper, proven option.
What Workers and Providers Should Do
If you’re an injured worker:
- Don’t assume brand-name drugs are better. They’re not.
- Ask your pharmacist: “Is this a generic? What’s the brand name?”
- If you feel the generic isn’t working, tell your doctor-but be ready to explain why, not just that you “prefer” the other one.
If you’re a provider:
- Know your state’s drug formulary. Check it every six months-rules change.
- Use the FDA’s Orange Book to verify therapeutic equivalence.
- Document medical necessity clearly. Vague statements like “patient preference” won’t hold up.
- Educate your patients. A 30-second explanation about bioequivalence can prevent weeks of confusion.
The system isn’t perfect. But it’s working. Generics save money, reduce waste, and deliver the same results. The only thing standing in the way is outdated thinking.
Are generic drugs really as effective as brand-name drugs in workers’ compensation?
Yes. The FDA requires generic drugs to have the same active ingredient, strength, dosage, and bioequivalence as their brand-name counterparts. This means they work the same way in the body. Studies show no meaningful difference in outcomes for workers’ compensation injuries. Over 89% of prescriptions in workers’ comp are now generic, and the system relies on their effectiveness.
Why do some doctors still prescribe brand-name drugs?
Some doctors prescribe brand-name drugs out of habit, lack of awareness, or because they believe patients expect them. Others may not be familiar with state-specific formularies. In states without strict substitution rules, brand-name drugs are still common. But in states with strong policies, like Tennessee and California, providers know they must document medical necessity-or the claim won’t be paid.
Can a worker refuse a generic drug and demand the brand name?
A worker can request the brand-name drug, but they usually can’t get it paid for by workers’ comp unless the doctor documents medical necessity. Insurers and PBMs won’t cover the cost unless there’s a valid clinical reason-like an allergy to a filler, or a documented failure of multiple generic versions. Patient preference alone is not enough.
What happens if a generic drug doesn’t work for me?
If a generic drug doesn’t work, the first step is to talk to your doctor. You may need to try a different generic-there are often multiple manufacturers. If those fail, your doctor can submit a request for a brand-name drug with clinical justification. This might include lab results, side effect logs, or prior treatment history. Most systems allow this process, but it requires documentation, not just a request.
Are there any drugs that can’t be substituted with generics?
Yes. Some drugs, especially biologics (like certain pain injections or immune-modulating drugs), don’t have true generic equivalents yet. Instead, biosimilars are being introduced, which are highly similar but not identical. Also, drugs with narrow therapeutic indexes-like warfarin or levothyroxine-require careful monitoring when switching. But even in these cases, generics or biosimilars are often used successfully with proper oversight.
How do I know if a drug is approved for generic substitution in my state?
Check your state’s workers’ compensation drug formulary, which is usually published by the state’s workers’ comp board or insurance commission. You can also ask your pharmacist or provider. The FDA’s Orange Book lists all approved generics and their therapeutic equivalence ratings. Most PBMs also provide online tools for providers to check formulary status in real time.





15 Comments
Look, I’ve been on workers’ comp for two years now, and let me tell you - the generic pill they gave me for my back pain? It did absolutely nothing. I switched from the brand, and suddenly I couldn’t even get out of bed. My doctor had to fight for three weeks just to get the original prescription approved. This system isn’t about saving money - it’s about ignoring real people’s pain. They treat us like numbers, not humans.
It is, without a shadow of a doubt, a profoundly concerning development that the pharmaceutical industry - and by extension, the entire workers’ compensation infrastructure - has, over the past decade, systematically prioritized cost-efficiency over clinical nuance, particularly when it comes to the substitution of generic medications in post-injury treatment protocols. While the FDA’s bioequivalence standards are, on paper, robust and well-structured, the reality on the ground reveals a deeply flawed implementation: pharmacists, under pressure from PBMs, routinely override physician discretion, and patients - many of whom have metabolic sensitivities, allergies to inactive ingredients, or unique pharmacokinetic profiles - are left to suffer in silence. The data may look good in spreadsheets, but the human cost? Unquantifiable.
This is a scam. A BIG ONE. The FDA? Controlled by Big Pharma. The PBMs? Owned by the same companies that make the brand drugs. They let generics in so they can charge MORE for the brand version later - then say ‘oh, we switched you to generic’ to look good. The ‘bioequivalence’? A lie. I’ve seen people go into seizures after switching. They hide the side effects. You think they test on real workers? Nah. They test on prisoners. And now they’re pushing this on injured people? Wake up. #PharmaControl
It is imperative to recognize that the systemic reliance on generic substitution, while economically rational, is fundamentally misaligned with the principles of individualized patient care. The assertion that generics are ‘just as effective’ is a gross oversimplification. Pharmacokinetic variability, differences in excipients, and inter-patient metabolic differences are not statistically insignificant - they are clinically critical. To mandate substitution without individualized assessment is not efficiency - it is medical negligence dressed up as fiscal responsibility. The fact that states like California have achieved 92.7% utilization does not prove efficacy - it proves compliance under coercion.
Bro, I used to work at a pharmacy. We got paid bonuses for swapping brand to generic. Like, every time we did it, we got $5. So yeah, we swapped. Even when the guy said ‘I always take the blue one.’ We swapped. And sometimes, the generic made him throw up. No one cared. They just said ‘next.’
The entire framework of generic substitution in workers’ compensation is a calculated maneuver orchestrated by insurance conglomerates and pharmacy benefit managers to externalize costs onto the injured worker. The FDA’s bioequivalence standards are not infallible - they are based on narrow, short-term pharmacokinetic studies conducted on healthy volunteers, not on individuals with chronic pain, liver dysfunction, or polypharmacy. The system does not protect patients - it protects balance sheets. The rise of biosimilars? A further escalation of this exploitation. This is not healthcare. This is corporate logistics.
Simple truth: if the generic didn’t work, it wouldn’t be approved. I’ve seen hundreds of workers switch from brand to generic - pain meds, anti-inflammatories, even nerve meds. 9 out of 10 didn’t notice a difference. The ones who did? Usually because they were used to the brand’s color or shape. Tell your doc if it’s not working - they can override it. But don’t just say ‘I like the blue pill.’ That’s not a medical reason. Just ask for help.
Let’s be real - this whole ‘generics are just as good’ narrative is a distraction. The real issue? The workers’ comp system doesn’t care if you heal. It cares if you stop filing claims. They push generics because it’s cheaper to deny care later than to pay for a brand drug now. And when you’re in pain? You’re not a patient. You’re a liability. They don’t want you better. They want you quiet.
I just want to say - I’ve been through this. I was injured at my warehouse job. I got the generic. It made me feel like I was floating. Like my brain was wrapped in cotton. I cried for three days. I didn’t tell anyone because I was scared they’d cut me off. But I finally told my nurse - and she cried with me. She said, ‘I’ve seen this before.’ It’s not about money. It’s about being seen. Please - if you’re feeling off on a generic? Speak up. You’re not crazy. You’re not weak. You’re just human.
So let me get this straight - we’re celebrating a system where a worker has to beg for a pill their body actually works with… and we call that progress? How about we start treating people like people instead of cost centers? Also - why are we still using 1980s logic in 2026? We have DNA testing. We have AI that can predict drug reactions. But instead? We’re still telling people to ‘just take the blue pill’ because it’s cheaper. Wow. We’re amazing.
Generics work. Doctors can override if needed. That’s the system. Stop making it a drama.
i had a back injury last year. switched to generic. no difference. saved the system $80. win win.
There is an ontological tension here - between the mechanistic reduction of human physiology to pharmacological equivalence, and the lived, embodied experience of pain, memory, and expectation. To reduce a person’s recovery to a bioequivalence curve is to erase the very subjectivity that defines healing. The FDA may validate molecular identity - but it cannot validate the soul’s recognition of a pill’s form, its color, its ritual. Perhaps the true failure is not in the generic - but in our refusal to see the patient as more than a data point.
India has been doing generics right for decades. We export 60% of the world’s generic drugs. Why? Because we don’t lie. We don’t overcharge. We don’t hide behind brand names. If Americans can’t handle a pill that works because it’s not branded - that’s their problem. Stop being so entitled. Your ‘blue pill’ isn’t sacred - it’s just a label. Learn from us.
They say generics are safe - but have you read the FDA’s own reports? The 2021 inspection of a major generic manufacturer in Hyderabad? 14 critical violations. Contaminated batches. Fake stability data. And they’re shipping those pills to injured workers in Ohio? Meanwhile, the same company that makes the generic? Also owns the brand-name version. They’re not saving money - they’re laundering profits. They want you to think you’re getting a deal. You’re getting a gamble. And if you get hurt? They’ll say ‘it was your body’s fault.’