Chronic Alcohol Use Disorder (AUD) isn’t just about drinking too much. It’s a medical condition where your brain and body become wired to need alcohol-even when it’s destroying your health, relationships, and life. You might still hold a job, show up for family events, or say you can quit anytime. But if you’ve tried to stop and couldn’t, or if you keep drinking despite blackouts, liver pain, anxiety, or depression, this isn’t a lack of willpower. It’s a brain disease. And it’s treatable.
What Happens to Your Body When You Drink Too Much for Too Long
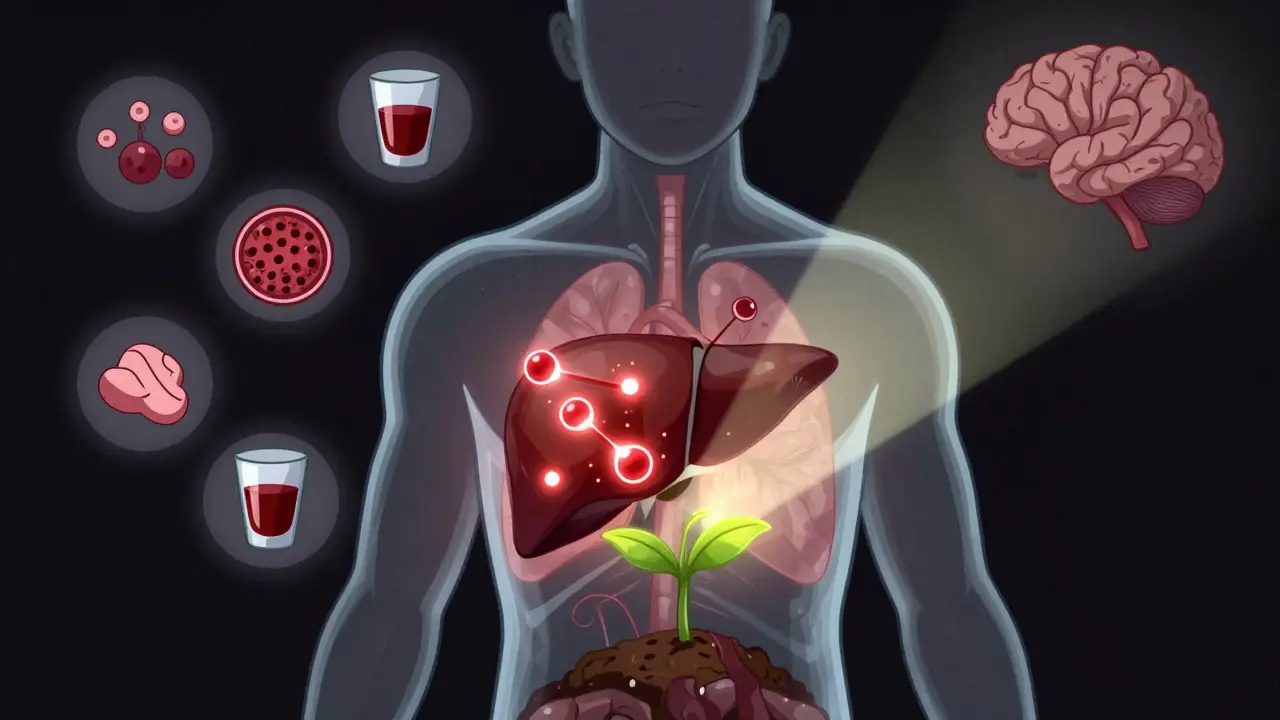
Your liver doesn’t just process alcohol-it gets battered by it. After years of heavy drinking, 90% of people develop fatty liver disease. That’s when fat builds up in liver cells. It’s reversible if you stop drinking. But if you keep going, inflammation kicks in: alcoholic hepatitis. Your liver swells, cells die, and you might start vomiting blood or turning yellow. Then comes cirrhosis-scar tissue replaces healthy liver tissue. Once cirrhosis sets in, your liver can’t regenerate. You’re at risk for liver failure or cancer. The CDC says alcohol contributes to over 60% of liver disease deaths in the U.S.
It’s not just your liver. Alcohol is a neurotoxin. It damages your brain’s communication pathways. Long-term drinkers often experience memory loss, trouble focusing, and even dementia. Thiamine (vitamin B1) deficiency hits 80% of people with chronic AUD. Without treatment, this leads to Wernicke’s encephalopathy: confusion, eye twitching, and loss of balance. Left untreated, it can become Korsakoff syndrome-a permanent form of amnesia.
Your heart doesn’t escape either. Heavy drinking raises your blood pressure, thickens your heart muscle, and triggers irregular rhythms like atrial fibrillation. That increases your stroke risk by 34% and your chance of heart attack by 40%. Alcohol also weakens your immune system. People with AUD are nearly three times more likely to get pneumonia. Even a simple cold can turn deadly.
And then there’s cancer. Alcohol breaks down into acetaldehyde, a known carcinogen. Heavy drinkers face a 5x higher risk of mouth and throat cancer, 3x higher risk of liver cancer, and a 12% increased risk of breast cancer for every daily drink. The American Cancer Society calls alcohol one of the top preventable causes of cancer.
How AUD Changes Your Mind
Alcohol starts as a depressant, but your brain adapts. At first, you feel relaxed. Then, you need more to get that same feeling. That’s tolerance. Soon, your brain stops making its own feel-good chemicals like dopamine and GABA. Now, you drink not to feel good-but to feel normal. Without alcohol, you get anxious, shaky, nauseous, or even have seizures. That’s physical dependence.
Mental health takes a hit too. About half of people with AUD also have depression or anxiety. Alcohol doesn’t cause these conditions-but it makes them worse. You drink to numb sadness, but then the crash makes you sadder. It’s a loop. Many people with AUD lose jobs, relationships, or homes. The National Institute on Alcohol Abuse and Alcoholism found that 60% of people with severe AUD report serious family conflict. One in five report being homeless at some point.
And it’s not just your life that suffers. Alcohol is involved in nearly one-third of all traffic deaths in the U.S. It fuels violence, crime, and suicide. Globally, alcohol kills 3 million people every year. That’s more than HIV, tuberculosis, and road injuries combined.
What Does AUD Look Like in Real Life?
There’s no single “alcoholic” look. You might be a parent who drinks wine every night to unwind. Or a veteran who uses whiskey to sleep. Or a college student who binges on weekends. AUD doesn’t care about your income, job, or background. The signs are more subtle than you think:
- Needing more drinks than before to feel the same effect
- Trying to cut back but failing
- Spending a lot of time drinking, recovering, or thinking about alcohol
- Missing work, school, or family events because of drinking
- Continuing to drink even when it causes health problems
- Getting sick or having withdrawal symptoms when you stop
If you recognize even a few of these, you’re not weak. You’re human. And you’re not alone. About 14.5 million adults in the U.S. have AUD. Yet only 19% get treatment.
Treatment Isn’t One-Size-Fits-All
Recovery starts with stopping. But quitting cold turkey can be deadly. Withdrawal from alcohol can cause seizures, hallucinations, or delirium tremens-a life-threatening condition. That’s why medical detox is often the first step. In a supervised setting, doctors monitor your vitals and give medications like benzodiazepines to keep you safe.
After detox, treatment shifts to healing the brain and changing behavior. Three FDA-approved medications help:
- Naltrexone (ReVia, Vivitrol): Blocks the pleasurable effects of alcohol. Reduces cravings by targeting opioid receptors in the brain.
- Acamprosate (Campral): Helps stabilize brain chemistry after stopping. Reduces anxiety and restlessness.
- Disulfiram (Antabuse): Makes drinking unpleasant-causes nausea, flushing, and rapid heartbeat if you consume alcohol.
Studies show combining medication with therapy works best. People who use both are 24% more likely to stay sober than those who use one alone.
Therapy That Actually Works
Not all therapy is the same. Here’s what the science says works:
- Cognitive Behavioral Therapy (CBT): Helps you spot triggers-stress, parties, loneliness-and replace drinking with healthier responses. One NIAAA study found CBT reduced heavy drinking days by 60%.
- Motivational Enhancement Therapy (MET): Focuses on resolving mixed feelings about quitting. It’s short, usually 3-4 sessions, and helps you find your own reasons to change.
- Contingency Management: Rewards you for staying sober-gift cards, vouchers, or other incentives. Proven effective in clinical trials.
Online therapy and apps are now part of mainstream treatment. The reSET app, approved by the FDA, guides users through CBT exercises and has helped 40.7% of users stay abstinent-nearly double the rate of those who didn’t use it.
Support Groups: Not Just for “Hardcore” Cases
Alcoholics Anonymous (AA) has been around since 1935. It’s not for everyone, but it works for many. Their 2014 survey showed 27% of members stayed abstinent after one year. Critics say the data isn’t perfect, but real people get better through it. The key isn’t the 12 steps-it’s the community. Talking to someone who’s been there? That’s powerful.
Other options include SMART Recovery, which uses science-based tools instead of spirituality, and Refuge Recovery, which blends mindfulness and Buddhism. The point isn’t which group you join-it’s that you’re not alone.

Emerging Treatments: What’s Next?
Science is moving fast. Transcranial Magnetic Stimulation (TMS), which uses magnetic pulses to calm overactive brain areas linked to cravings, showed 50% abstinence rates in a 2022 JAMA Psychiatry trial. That’s promising for people who haven’t responded to other treatments.
There’s also research into psychedelics like psilocybin. Early studies suggest a single session, combined with therapy, can reduce heavy drinking for months. The FDA has granted breakthrough status to some of these trials.
And it’s not just about stopping. Recovery is about rebuilding. Nutritional support, exercise, sleep hygiene, and reconnecting with loved ones all play a role. Many people regain liver function after 6-12 months of abstinence. Some even reverse early-stage cirrhosis.
Can You Really Get Better?
Yes. Not everyone does. But many do. Recovery isn’t about perfection. It’s about progress. One day at a time. One drink avoided. One therapy session attended. One phone call made to a sponsor.
The myth that AUD is a moral failure is the biggest barrier to treatment. It’s not. It’s a medical condition with biological, psychological, and social roots. And like diabetes or hypertension, it can be managed-with the right tools, support, and time.
If you’re reading this and thinking, “That’s me,” you’re not broken. You’re sick. And you deserve help.
Is chronic alcohol use disorder the same as alcoholism?
Yes. Alcoholism is the informal term for what doctors now call Alcohol Use Disorder (AUD). The DSM-5, the standard diagnostic manual used by clinicians, combined alcohol abuse and dependence into one condition called AUD, with mild, moderate, and severe levels. Severe AUD is what most people mean when they say “alcoholism.”
Can your liver recover after years of heavy drinking?
It depends. Fatty liver and early-stage alcoholic hepatitis can reverse within weeks or months of stopping alcohol. Cirrhosis is harder to undo. Once scar tissue forms, it doesn’t disappear. But stopping drinking can stop further damage and let the liver heal as much as it can. Some people with advanced cirrhosis live for years after quitting, especially if they get medical care.
Do I need to go to rehab to quit drinking?
Not always. Some people quit successfully with outpatient therapy, medication, and support groups. But if you’ve been drinking heavily for years, or you’ve had withdrawal symptoms before, medically supervised detox is strongly recommended. Quitting cold turkey can be dangerous-or deadly. Rehab gives you structure, safety, and support during the hardest part.
Are AUD medications just replacing one addiction with another?
No. Medications like naltrexone and acamprosate don’t cause euphoria or dependence. They help reduce cravings and stabilize brain chemistry so you can focus on therapy and rebuilding your life. Think of them like insulin for diabetes-they correct a biological imbalance, not create a new one.
How long does treatment for AUD take?
There’s no set timeline. Detox takes days to weeks. Therapy often lasts 3-6 months or longer. Many people stay in support groups for years. Recovery isn’t a finish line-it’s a lifelong practice. The goal isn’t to “cure” AUD, but to manage it so it doesn’t control your life.
Can I drink moderately after treatment?
For most people with severe AUD, abstinence is the safest and most effective path. Research shows that even small amounts of alcohol can trigger relapse. The brain remembers the reward pathway too well. Some people try controlled drinking, but the success rate is low. If you’ve lost control before, the risk of returning to heavy use is high. Abstinence gives your brain the best chance to heal.
What Comes Next?
If you’re ready to stop, start by talking to your doctor. Ask about screening tools like the AUDIT test. Get blood work done to check your liver and vitamin levels. Ask about medication options. Look up local support groups. You don’t have to do this alone.
If you’re worried about someone else, don’t wait for them to hit rock bottom. Offer help-not judgment. Say: “I care about you. I’ve noticed you’ve been drinking more. I’m here if you want to talk.” That’s often the first step to recovery.
Chronic Alcohol Use Disorder doesn’t define you. But how you respond to it? That does. And the right help makes all the difference.





10 Comments
Been sober 3 years now. Didn’t think I’d make it past 30. The liver thing? Real. My ALT levels were through the roof. Now they’re normal. Not magic-just time and stopping.
One day at a time. That’s all I ever had to do.
People need to STOP making excuses!!! It’s not a ‘disease’-it’s a choice! You choose to drink! You choose to ignore your family! You choose to ruin your body! Why do we keep coddling this?!? I’ve seen people die from this-literally! And they were just… weak! No one held a gun to their head! Why is this ‘treatable’ and not ‘fixable’?!
Hey-just wanted to say thank you for writing this. I’ve been sitting on this for years. My dad had AUD. He never got help. He died at 52. I’m 34 now. I started therapy last year. The part about thiamine? That was him. He couldn’t remember my wedding. I didn’t know why until I read this.
There’s hope. Even if it feels like there isn’t.
It is important to emphasize that the medical model of addiction, while scientifically robust, must be integrated with psychosocial support. The pharmacological interventions you referenced-naltrexone, acamprosate, and disulfiram-are adjunctive to behavioral therapy. The data from the NIAAA supports multimodal treatment as the gold standard. Furthermore, the neuroplasticity of the prefrontal cortex allows for significant recovery, even in chronic cases, provided abstinence is maintained.
my cousin did the whole detox + aa thing and it worked for him, but honestly? the thing that kept him going was his dog. he’d come home, collapse on the couch, and the dog would just stare at him like ‘you’re not doing this again, buddy.’
weird, right? but it worked.
I’m so glad someone wrote this with such clarity. I’ve watched friends spiral and felt helpless. I’ve also seen people rise. It’s not about being strong-it’s about being supported. You’re not alone. Not anymore.
In many Eastern traditions, suffering is not viewed as a moral failing, but as a signal-an invitation to transform. Alcohol use disorder, in this light, is not a defect of character, but a misalignment between the self and its deeper needs. The body screams for peace, and the mind reaches for a bottle because it has forgotten how to sit still. Healing, then, is not merely cessation, but reintegration. The path is long, but it is walked by many before us.
lol so now alcoholism is a brain disease but if you’re overweight it’s just ‘lazy’? funny how the medical community picks and chooses what’s ‘biological’ and what’s ‘personal responsibility’.
also-psilocybin? really? next you’ll say we should give people LSD to fix their tax problems.
They’re hiding the truth. Big Pharma pushed this ‘disease’ narrative so they could sell you pills. Naltrexone? It’s a cover-up. The real fix? Stop drinking. No meds. No therapy. Just quit. Why won’t they tell you that? Because they make billions off your suffering.
Also-did you know the CDC is funded by alcohol companies? That’s why they say it’s ‘preventable’-so you think you’re safe if you just drink ‘a little’.
There is a profound cultural irony here: Western medicine, in its clinical detachment, has pathologized a deeply human struggle-our collective desire to escape discomfort-while simultaneously commodifying its solution. The very institutions that diagnose AUD as a ‘brain disease’ are the same ones that profit from its treatment. We have turned a spiritual crisis into a pharmaceutical product line. The 12 steps, the mindfulness apps, the TMS machines-they are all modern rituals for a society that fears silence. The real cure is not in a pill or a session, but in the courage to sit with your pain without reaching for the bottle. And that? That’s not something you can prescribe. It’s something you must choose. Every day. Again. And again.